
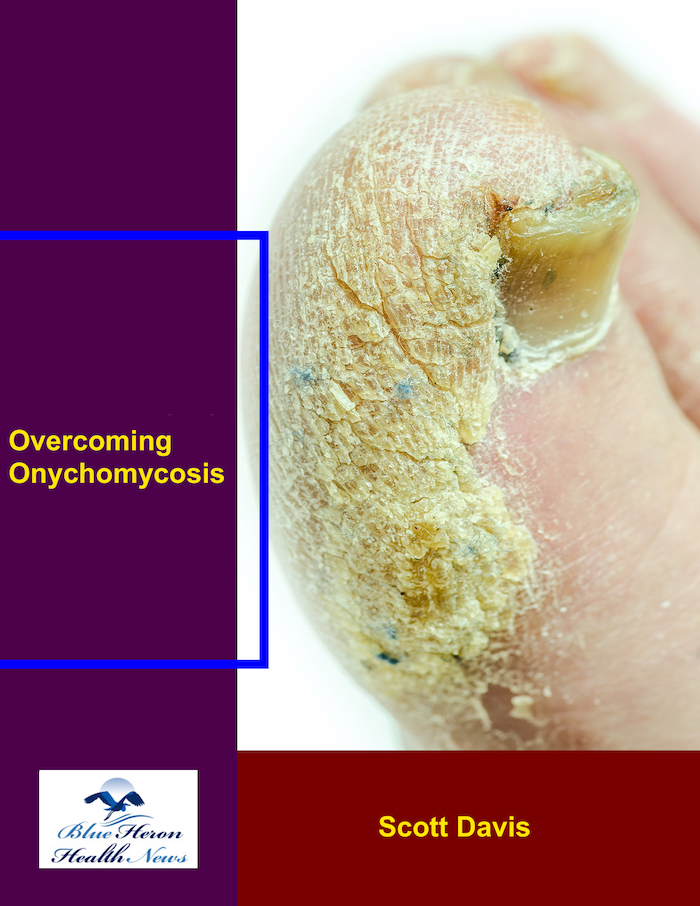
Overcoming Onychomycosis™ By Scott Davis If you want a natural and proven solution for onychomycosis, you should not look beyond Overcoming Onychomycosis. It is easy to follow and safe as well. You will not have to take drugs and chemicals. Yes, you will have to choose healthy foods to treat your nail fungus. You can notice the difference within a few days. Gradually, your nails will look and feel different. Also, you will not experience the same condition again!
What is the prevalence of hypothyroidism after neck surgery or radioiodine therapy, supported by treatment outcome studies, and how do surgical patients compare with nonsurgical patients?
The prevalence of hypothyroidism following neck surgery or radioiodine therapy is remarkably high, with both interventions representing primary iatrogenic causes of an underactive thyroid. Treatment outcome studies consistently demonstrate that while both paths frequently lead to the same destination of lifelong thyroid hormone replacement, the journey, timeline, and clinical nuances for surgical and nonsurgical patients are profoundly different. Surgical intervention, particularly total thyroidectomy, results in an immediate and absolute hypothyroid state, whereas radioiodine therapy induces a more gradual, insidious decline in thyroid function over months to years. A comparison of these patient populations reveals distinct differences in the predictability, onset, and management of their subsequent hypothyroidism.
Hypothyroidism Following Neck Surgery 🔪
Neck surgery encompasses a variety of procedures that can impact the thyroid gland, either intentionally or incidentally. The prevalence of postoperative hypothyroidism is entirely dependent on the nature and extent of the surgery performed. The most definitive procedure is a total thyroidectomy, the complete removal of the thyroid gland, which is often performed for thyroid cancer, large goiters, or severe Graves’ disease. In this scenario, the prevalence of hypothyroidism is absolute: one hundred percent. The outcome is not a risk but a certainty. Since the body’s sole source of thyroid hormone production has been removed, patients are rendered immediately and permanently hypothyroid. Treatment outcome studies are less about prevalence and more about the management of this expected state. Clinical practice dictates the immediate initiation of lifelong levothyroxine replacement therapy, with the goal of normalizing serum Thyroid Stimulating Hormone (TSH) levels and rendering the patient euthyroid (having normal thyroid function).
The clinical picture becomes more variable following a hemithyroidectomy, or thyroid lobectomy, where only one lobe of the thyroid is removed. This procedure is common for solitary thyroid nodules or small, low-risk thyroid cancers confined to one side. Here, the remaining lobe has the potential to produce enough hormone to compensate for the loss of the other. However, a significant portion of patients fail to achieve this compensation. Treatment outcome studies and large meta-analyses place the prevalence of hypothyroidism after hemithyroidectomy in a wide range, typically between 20% and 50%. The variability is influenced by several key pre-operative factors. For instance, studies have conclusively shown that a higher pre-operative TSH level, even within the normal range, is a strong predictor of post-surgical hypothyroidism. The presence of anti-thyroid peroxidase (TPO) antibodies, indicative of an underlying autoimmune thyroiditis (Hashimoto’s disease), is another major risk factor, as the autoimmune process will continue to affect the remaining thyroid tissue. Therefore, while not a certainty, the risk is substantial, and patients require careful long-term monitoring of their thyroid function.
Hypothyroidism can also be an unintended consequence of other neck surgeries. During a parathyroidectomy, performed to treat hyperparathyroidism, the surgeon must carefully work around the thyroid gland. In some cases, the blood supply to the thyroid may be compromised, or a portion of the gland may need to be removed to access the parathyroid glands, leading to subsequent hypothyroidism. Similarly, anterior cervical spine surgery, a common neurosurgical procedure, involves an incision in the front of the neck that requires retraction of the thyroid gland. This manipulation can lead to inflammation, devascularization, or direct injury. Outcome studies on these incidental impacts show a lower but still significant prevalence of hypothyroidism, often ranging from 5% to 15%, a risk that necessitates post-operative awareness and screening.
Hypothyroidism Following Radioiodine Therapy ☢️
Radioiodine (RAI) therapy is a nonsurgical, definitive treatment for hyperthyroidism, most commonly caused by Graves’ disease or toxic nodular goiter. The treatment involves swallowing a capsule containing radioactive iodine-131. The thyroid gland naturally absorbs almost all of the iodine in the body to make thyroid hormone. The RAI is therefore selectively taken up by the overactive thyroid cells, where it emits radiation that destroys them over a period of weeks to months. While highly effective at curing hyperthyroidism, this cellular destruction almost inevitably leads to permanent hypothyroidism.
For patients with Graves’ disease, an autoimmune condition where the entire gland is overactive, RAI therapy is designed to ablate the majority of the thyroid tissue. Consequently, the prevalence of subsequent hypothyroidism is extremely high. Treatment outcome studies demonstrate a clear time-dependent effect. While only about 20-40% of patients may become hypothyroid within the first year, the cumulative incidence steadily rises over time. Multiple long-term follow-up studies show that by five years post-treatment, 70-80% of patients are hypothyroid, and the rate can exceed 90% after ten to twenty years. For this reason, hypothyroidism is considered an expected and intended outcome of RAI therapy for Graves’ disease, aimed at replacing the unpredictable and difficult-to-manage state of hyperthyroidism with the stable and easily managed state of hypothyroidism.
The prevalence can be slightly different for patients with toxic multinodular goiter or a solitary toxic adenoma. In these conditions, only specific nodules within the thyroid are overactive, while the surrounding thyroid tissue is often suppressed. The goal of RAI therapy is to target and destroy these “hot” nodules. Because the overactive nodules absorb the majority of the radioiodine, the surrounding normal tissue is often spared from the full destructive effect. As a result, the prevalence of hypothyroidism is generally lower than in Graves’ disease patients. Outcome studies for toxic nodular goiter report hypothyroidism rates ranging from 20% to 60% in the years following treatment. While the risk is lower, it remains substantial and lifelong monitoring is still essential.
A Comparative Analysis: Surgical vs. Nonsurgical Patients ⚖️
When comparing patients who become hypothyroid from surgery versus those treated with radioiodine, the differences in clinical trajectory are stark. The first major distinction is the onset and predictability of hypothyroidism. For a total thyroidectomy patient, the onset is immediate and the outcome is 100% predictable. They leave the hospital with a prescription for levothyroxine and a clear management plan. In contrast, the RAI patient enters a period of clinical uncertainty. Their thyroid function will decline gradually over an unpredictable timeline, necessitating regular blood tests every few months for the first year and annually thereafter. This creates a prolonged “watchful waiting” period, where patients may experience subtle symptoms of hypothyroidism for months before their TSH levels officially cross the diagnostic threshold.
This leads to the second difference: the patient experience and management. The surgical patient’s journey is characterized by the acute challenges of surgery and recovery, followed by the straightforward, albeit lifelong, task of taking a daily pill and having annual blood tests. The RAI patient avoids surgery but must navigate a slower, more ambiguous transition. They may experience a period where their thyroid function swings between hyperthyroid, euthyroid, and ultimately hypothyroid, which can be emotionally and physically taxing. The onus is on continuous long-term monitoring to detect the eventual onset of hypothyroidism, which can occur one year, five years, or even two decades after the initial treatment.
Finally, the underlying mechanism and final state of the gland differ. Surgery involves the physical removal of the gland, leaving no thyroid tissue behind (in a total thyroidectomy). RAI therapy leaves behind a gland that is still physically present but has been functionally destroyed by radiation, becoming a small, fibrotic, non-functional remnant. While this distinction has little impact on the final need for hormone replacement, it reflects the fundamentally different approaches: one of anatomical removal and the other of functional ablation. In summary, while both surgery and radioiodine are highly effective treatments that frequently result in hypothyroidism, they place patients on very different clinical paths. The surgical route offers certainty and an immediate management plan at the cost of an invasive procedure, while the nonsurgical radioiodine route offers a less invasive option but introduces a prolonged period of unpredictability and a need for vigilant, long-term surveillance.
Overcoming Onychomycosis™ By Scott Davis If you want a natural and proven solution for onychomycosis, you should not look beyond Overcoming Onychomycosis. It is easy to follow and safe as well. You will not have to take drugs and chemicals. Yes, you will have to choose healthy foods to treat your nail fungus. You can notice the difference within a few days. Gradually, your nails will look and feel different. Also, you will not experience the same condition again!

I’m Mr.Hotsia, sharing 30 years of travel experiences with readers worldwide. This review is based on my personal journey and what I’ve learned along the way. Learn more |