
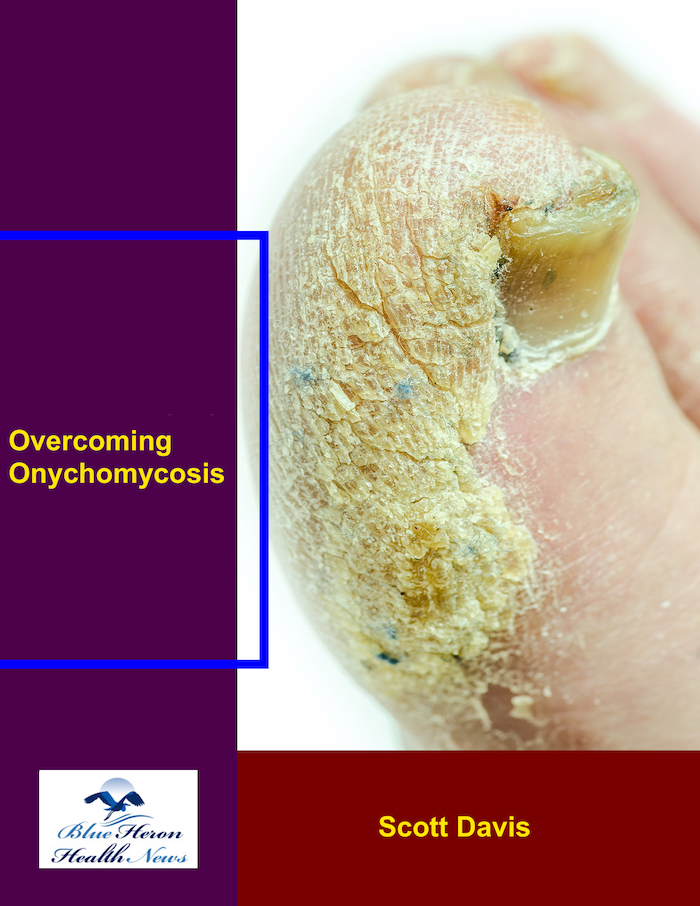
Overcoming Onychomycosis™ By Scott Davis If you want a natural and proven solution for onychomycosis, you should not look beyond Overcoming Onychomycosis. It is easy to follow and safe as well. You will not have to take drugs and chemicals. Yes, you will have to choose healthy foods to treat your nail fungus. You can notice the difference within a few days. Gradually, your nails will look and feel different. Also, you will not experience the same condition again!
What is the prevalence of hypothyroidism in Middle Eastern refugee populations, supported by humanitarian health data, and how do displaced populations compare with host populations?
🩺 The Hidden Burden: Hypothyroidism in Middle Eastern Refugee Populations 🩺
The prevalence of hypothyroidism in Middle Eastern refugee populations is a significant but often under-documented public health challenge, representing a hidden burden within the broader crisis of non-communicable diseases (NCDs) in displaced communities. While precise, large-scale epidemiological statistics comparable to stable national surveys are scarce due to the inherent difficulties of conducting systematic research in crisis settings, the available humanitarian health data and an understanding of the risk factors involved strongly suggest that hypothyroidism is a common and growing concern. The condition is often subsumed under the larger category of “endocrine disorders” in humanitarian reports, but clinical evidence from the field confirms it as a frequent diagnosis. The prevalence is driven by a confluence of factors, including the disruption of pre-existing care, the profound physiological and psychological stress of displacement, and potential nutritional deficiencies, creating a unique and challenging health landscape for this vulnerable population.
Forced displacement creates a perfect storm of risk factors for both the development and the exacerbation of hypothyroidism. Many refugees, particularly those from countries like Syria which had a relatively robust healthcare system prior to conflict, were already diagnosed with hypothyroidism (most commonly autoimmune Hashimoto’s thyroiditis) and were stable on lifelong thyroid hormone replacement therapy, such as levothyroxine. Displacement abruptly severs this continuity of care. Prescriptions are lost, access to pharmacies and physicians is cut off, and the daily priority shifts from managing a chronic illness to ensuring basic survival. This leads to a large population of individuals with pre-existing disease who are suddenly untreated, causing them to develop the overt and debilitating symptoms of hypothyroidism, such as profound fatigue, weight gain, depression, and cognitive slowing.
Furthermore, the experience of displacement itself can trigger or worsen thyroid dysfunction. The immense and unremitting chronic stress associated with trauma, loss, and the precariousness of refugee life has a direct impact on the endocrine system. Stress can dysregulate the hypothalamic-pituitary-adrenal (HPA) axis, which in turn can disrupt the hypothalamic-pituitary-thyroid (HPT) axis that controls thyroid hormone production. More importantly, chronic stress is a known trigger for autoimmune diseases. It can accelerate the autoimmune attack on the thyroid gland in genetically susceptible individuals, potentially initiating Hashimoto’s thyroiditis in those who may not have otherwise developed it, or worsening the condition in those with subclinical disease. Nutritional deficiencies also play a critical role. While iodine deficiency, the classic cause of goiter and hypothyroidism, has been largely controlled in the Middle East through salt iodization programs, refugee populations relying on inconsistent food aid may be at risk for inadequate intake. Deficiencies in other micronutrients essential for thyroid function, such as selenium and zinc, can also occur due to a limited and non-diverse diet in camps or urban poverty settings.
📊 Insights from Humanitarian Health Data 📊
Direct, population-wide prevalence statistics for hypothyroidism among Middle Eastern refugees are not readily available from major humanitarian organizations, as their data collection priorities are often focused on acute conditions, infectious disease outbreaks, and broader categories of NCDs like cardiovascular disease and diabetes. However, the data that is available consistently points to endocrine disorders as a significant and growing component of the NCD burden. Reports from the United Nations High Commissioner for Refugees (UNHCR) and the World Health Organization (WHO) on the health status of Syrian refugees in host countries like Jordan, Lebanon, and Turkey frequently highlight that “endocrine, nutritional, and metabolic diseases” account for a substantial portion of all NCD-related consultations in humanitarian clinics. Within this category, hypothyroidism and diabetes are the most commonly managed conditions.
Smaller-scale, focused studies and clinic-based reports provide a more granular, albeit not generalizable, view of the problem. For example, a clinical audit conducted in a primary health care center serving Syrian refugees in Lebanon might reveal that hypothyroidism is one of the top five most common chronic conditions for which medication is dispensed. These on-the-ground reports from organizations like Doctors Without Borders (MSF) and other NGOs confirm that managing thyroid disease is a routine part of their work in the region. They encounter patients who have run out of their essential levothyroxine medication, as well as newly diagnosed cases in patients presenting with the classic symptoms of fatigue and depression. This clinic-based data, while not providing a precise prevalence rate, serves as crucial evidence. It demonstrates that hypothyroidism is not a rare or insignificant issue but a persistent clinical reality that requires a consistent supply of diagnostics and medication within the humanitarian responsea response that has historically been more geared towards acute care than the long-term management of chronic disease.
⚖️ A Comparative Analysis: Displaced vs. Host Populations ⚖️
When comparing the prevalence and management of hypothyroidism in displaced refugee populations versus their host communities in countries like Jordan, Lebanon, and Turkey, it is essential to consider both the baseline risk and the unique impact of the displacement crisis.
The host populations in the Middle East already have a significant baseline prevalence of hypothyroidism, particularly autoimmune Hashimoto’s thyroiditis. There is a known genetic predisposition to autoimmune diseases in the region, and widespread vitamin D deficiency, a potential risk factor for autoimmunity, is also common. Therefore, hypothyroidism is a familiar and common diagnosis in the primary care systems of these countries. A citizen or long-term resident of a host country, however, typically has access to a stable, functioning healthcare system. They can receive a diagnosis, get a renewable prescription for levothyroxine, and have regular follow-up appointments to monitor their thyroid-stimulating hormone (TSH) levels and adjust their dosage. While there may be economic barriers for some, the infrastructure for continuous care exists.
The displaced refugee population, while sharing a similar genetic and regional predisposition to thyroid disease as their hosts, faces a dramatically different reality. The critical difference is the profound disruption of access to healthcare and the overwhelming burden of stress. A Syrian refugee, for example, is likely to have a similar underlying risk for Hashimoto’s as a Jordanian citizen. However, the refugee’s ability to manage that risk is severely compromised. Their prevalence of undiagnosed, untreated, or poorly managed hypothyroidism is almost certainly higher than in the host population. The barriers they face are immense: the cost of consultations and medications is often prohibitive, humanitarian clinics are frequently overwhelmed and may not be equipped for the nuanced management of endocrine disorders, and the lack of legal status or documentation can prevent access to national health services. Furthermore, the constant, severe stress of their situation acts as an additional physiological insult, potentially increasing the incidence of the disease. Therefore, while the total underlying prevalence of thyroid autoimmunity might be comparable between the two groups, the prevalence of symptomatic, clinically significant, and untreated hypothyroidism is expected to be substantially higher in the refugee population. They suffer not just from the disease itself, but from the collapse of the systems required to manage it.
Overcoming Onychomycosis™ By Scott Davis If you want a natural and proven solution for onychomycosis, you should not look beyond Overcoming Onychomycosis. It is easy to follow and safe as well. You will not have to take drugs and chemicals. Yes, you will have to choose healthy foods to treat your nail fungus. You can notice the difference within a few days. Gradually, your nails will look and feel different. Also, you will not experience the same condition again!

I’m Mr.Hotsia, sharing 30 years of travel experiences with readers worldwide. This review is based on my personal journey and what I’ve learned along the way. Learn more |