
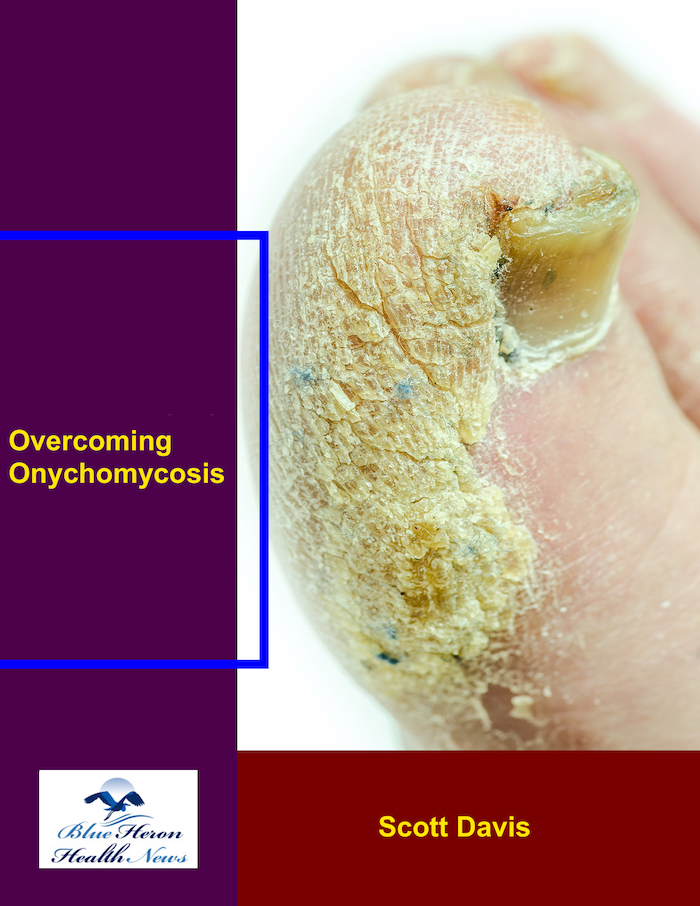
Overcoming Onychomycosis™ By Scott Davis If you want a natural and proven solution for onychomycosis, you should not look beyond Overcoming Onychomycosis. It is easy to follow and safe as well. You will not have to take drugs and chemicals. Yes, you will have to choose healthy foods to treat your nail fungus. You can notice the difference within a few days. Gradually, your nails will look and feel different. Also, you will not experience the same condition again!
How does chronic lithium therapy affect hypothyroidism prevalence, supported by psychiatric population studies, and how do outcomes compare with non-lithium users?
Chronic lithium therapy, a cornerstone in the management of bipolar disorder and other mood disorders, profoundly affects the prevalence of hypothyroidism, establishing a well-documented and clinically significant side effect. An extensive body of evidence from psychiatric population studies confirms that long-term lithium use dramatically increases the risk of developing both overt and subclinical hypothyroidism. When the outcomes for these patients are compared with those of psychiatric patients not using lithium, the data reveals a stark contrast, highlighting lithium as a potent independent risk factor for thyroid dysfunction. The relationship between this essential medication and the thyroid gland is a critical area of clinical focus, necessitating vigilant monitoring and management to ensure patient safety and therapeutic success.
The Mechanism of Disruption: How Lithium Impairs the Thyroid Gland ⚙️
The thyroid gland’s susceptibility to lithium stems from the ion’s chemical similarity to sodium and iodine. Because of this resemblance, lithium is actively transported into and concentrated within thyroid follicular cells, reaching levels three to four times higher than in the blood plasma. Once inside the gland, lithium exerts a multifaceted inhibitory effect on the entire process of thyroid hormone synthesis and secretion, effectively acting as a goitrogen. Its primary mechanism of action is the inhibition of thyroid hormone release from the colloid stores within the gland. It disrupts the colloid’s endocytosis and the proteolytic cleavage of thyroglobulin, which is the final step required to release active thyroxine (T4) and triiodothyronine (T3) into the bloodstream. This blockade is a significant and immediate effect of lithium exposure.
Beyond inhibiting hormone release, lithium also interferes with earlier stages of hormone production. It reduces the thyroid’s ability to take up iodine from the blood, a crucial first step in synthesizing hormones. Furthermore, it impairs the organification process, where iodine is incorporated into tyrosine residues on the thyroglobulin molecule, and inhibits the coupling of these iodotyrosine molecules to form T4 and T3. This multi-step disruption ensures that both the creation and secretion of thyroid hormones are suppressed. Over time, the pituitary gland detects falling levels of thyroid hormone and responds by increasing its output of Thyroid Stimulating Hormone (TSH) in an effort to compel the thyroid to produce more. This sustained elevation in TSH can lead to the physical enlargement of the thyroid gland, known as a goiter, and is the biochemical hallmark of developing hypothyroidism. Moreover, there is compelling evidence that lithium can trigger or unmask autoimmune thyroid disease, such as Hashimoto’s thyroiditis, by possibly altering immune responses and leading to the production of anti-thyroid peroxidase (TPO) antibodies.
The Weight of Evidence: Hypothyroidism Prevalence in Psychiatric Population Studies 📊
Decades of research have firmly established the high prevalence of hypothyroidism among patients on chronic lithium therapy. The findings from numerous cohort studies, cross-sectional analyses, and meta-analyses converge on this point, although the exact prevalence rates vary depending on the study population, duration of lithium use, and the diagnostic criteria used. The most consistently reported finding is the development of overt, or clinical, hypothyroidism, which is characterized by an elevated TSH and a low free T4 level. Large-scale studies of psychiatric populations on long-term lithium treatment report a prevalence of overt hypothyroidism ranging from 8% to as high as 20%. This represents a significant portion of treated individuals who will require thyroid hormone replacement therapy to manage their symptoms, which can include fatigue, weight gain, depression, and cognitive slowing, symptoms that can often overlap with and complicate the underlying psychiatric disorder.
Even more common than overt hypothyroidism is the development of subclinical hypothyroidism, a milder form of thyroid dysfunction defined by an elevated TSH level in the presence of a normal free T4 level. The prevalence of subclinical hypothyroidism in the lithium-treated population is even higher, with many studies reporting rates between 20% and 30%. While patients may not have overt symptoms, this subclinical state is a significant risk factor for progression to clinical hypothyroidism and has been associated with subtle mood instability and poorer response to antidepressants. The risk is not uniform across all patients. Population studies have identified several key risk factors that dramatically increase an individual’s susceptibility. The most prominent risk factor is female gender, with women on lithium being three to five times more likely to develop hypothyroidism than men. Another major predictor is the presence of pre-existing anti-TPO antibodies, indicating an underlying autoimmune predisposition. Patients who are antibody-positive before starting lithium have a substantially accelerated and increased risk of developing thyroid failure once therapy begins. The risk also increases with the duration of lithium treatment and is higher in individuals with a family history of thyroid disease.
A Tale of Two Cohorts: Lithium Users vs. Non-Lithium Users ⚖️
To truly understand the magnitude of lithium’s effect, it is essential to compare the outcomes in lithium-treated patients with those in a similar cohort of psychiatric patients not taking the medication. Many mood disorders, including bipolar disorder, are themselves associated with a slightly increased background risk of thyroid dysfunction, particularly autoimmune thyroiditis. Therefore, using a control group of non-lithium-using psychiatric patients helps to isolate the specific impact of the drug. Comparative studies consistently and unequivocally demonstrate that lithium confers a risk of hypothyroidism that is far above the baseline risk associated with the psychiatric illness alone.
In studies comparing patients with bipolar disorder on lithium to those on other mood stabilizers like valproate or antipsychotics, the difference in hypothyroidism prevalence is stark. For example, a typical comparative study might find a hypothyroidism prevalence of around 20% in the lithium group, compared to only 3-5% in the non-lithium control group. This represents a roughly four- to six-fold increase in risk directly attributable to lithium. This finding holds true for both overt and subclinical hypothyroidism. The incidence, or the rate of new cases developing over time, is also dramatically higher. Longitudinal studies that follow patients over many years show a continuous and steady emergence of new cases of hypothyroidism in the lithium-treated group, while the incidence in the control group remains low and stable.
The clinical outcomes and management trajectory also diverge significantly. For a non-lithium user with a mood disorder, hypothyroidism, when it occurs, is typically managed as a separate comorbidity, often arising from an autoimmune process like Hashimoto’s disease. For the lithium user, hypothyroidism is considered a direct and predictable side effect of their primary psychiatric treatment. This knowledge fundamentally changes the clinical approach. It mandates proactive and routine screening as a standard of care. Clinical guidelines universally recommend obtaining a baseline TSH and anti-TPO antibody test before initiating lithium, followed by routine TSH monitoring every six to twelve months for the entire duration of therapy. This allows for the early detection and treatment of thyroid dysfunction, often before significant symptoms develop. Fortunately, the management of lithium-induced hypothyroidism is straightforward. It is effectively treated with levothyroxine (synthetic T4) supplementation. Crucially, the development of hypothyroidism is not an indication to stop lithium therapy. The mood-stabilizing benefits of lithium are often so profound and essential for the patient’s mental health that it is almost always preferable to continue the lithium and simply treat the hypothyroidism with hormone replacement, a safe and effective combination. In conclusion, the evidence from psychiatric population studies is overwhelming: chronic lithium therapy is a powerful trigger for hypothyroidism, with a prevalence that dwarfs that seen in non-lithium-using psychiatric patients. This elevated risk is a predictable and manageable aspect of treatment, underscoring the indispensable role of vigilant thyroid monitoring in ensuring the long-term safety and well-being of patients who rely on this life-changing medication.
Overcoming Onychomycosis™ By Scott Davis If you want a natural and proven solution for onychomycosis, you should not look beyond Overcoming Onychomycosis. It is easy to follow and safe as well. You will not have to take drugs and chemicals. Yes, you will have to choose healthy foods to treat your nail fungus. You can notice the difference within a few days. Gradually, your nails will look and feel different. Also, you will not experience the same condition again!

I’m Mr.Hotsia, sharing 30 years of travel experiences with readers worldwide. This review is based on my personal journey and what I’ve learned along the way. Learn more |