
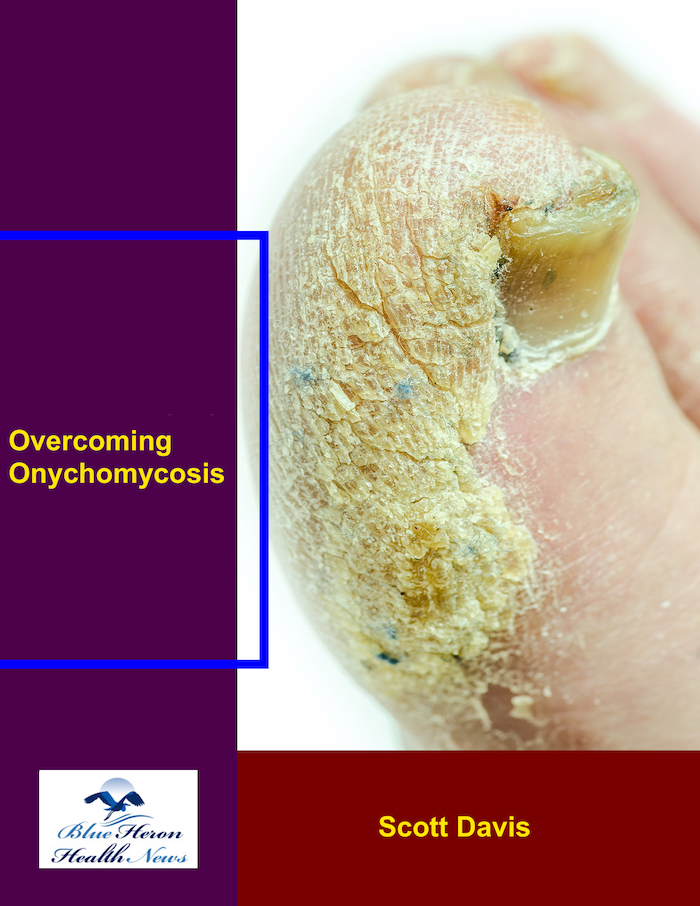
Overcoming Onychomycosis™ By Scott Davis If you want a natural and proven solution for onychomycosis, you should not look beyond Overcoming Onychomycosis. It is easy to follow and safe as well. You will not have to take drugs and chemicals. Yes, you will have to choose healthy foods to treat your nail fungus. You can notice the difference within a few days. Gradually, your nails will look and feel different. Also, you will not experience the same condition again!
What is the prevalence of hypothyroidism in Down syndrome, supported by genetic cohort data, and how do outcomes compare with the general population?
The prevalence of hypothyroidism in individuals with Down syndrome is extraordinarily high, representing one of the most common medical comorbidities associated with this genetic condition. Supported by a wealth of data from genetic cohort studies and longitudinal research, it is unequivocally established that people with Down syndrome experience a dramatically increased risk of all forms of thyroid dysfunction throughout their entire lifespan. This risk is not merely a slight statistical increase; it is a profound and fundamental aspect of the pathophysiology of Trisomy 21. When their outcomes are compared with those of the general population, the differences in prevalence, age of onset, underlying cause, and clinical management are stark, mandating a uniquely vigilant approach to screening and care for this vulnerable group.
The Genetic and Immunological Foundation of Thyroid Risk 🧬
The root cause of the heightened susceptibility to hypothyroidism in Down syndrome lies within the genetic makeup of Trisomy 21 itself. The presence of an extra copy of chromosome 21 leads to the overexpression of numerous genes, several of which play critical roles in regulating the immune system. This genetic imbalance creates a state of inherent immune dysregulation, characterized by a complex mix of both immunodeficiency and autoimmunity. This predisposition to autoimmunity is the primary driver behind the high rates of acquired hypothyroidism. Cohort studies consistently show a significantly higher prevalence of thyroid-specific autoantibodies, such as anti-thyroid peroxidase (TPO) and anti-thyroglobulin (Tg) antibodies, in individuals with Down syndrome. These antibodies are the hallmark of autoimmune thyroiditis, also known as Hashimoto’s disease, a condition where the body’s own immune system mistakenly attacks and systematically destroys the thyroid gland.
The overexpression of genes on chromosome 21, such as the autoimmune regulator gene (AIRE) and various interferon-related genes, is thought to disrupt central and peripheral tolerance, the mechanisms that prevent the immune system from attacking self-tissues. This creates an environment where the thyroid gland, for reasons not yet fully understood, becomes a prime target. Therefore, the genetic blueprint of Down syndrome itself launches a lifelong, elevated risk of autoimmune-mediated thyroid failure. This is fundamentally different from the general population, where the development of autoimmune thyroid disease is influenced by a more complex interplay of multiple genetic and environmental factors, without a single, powerful predisposing chromosomal condition.
A Lifelong Journey: Hypothyroidism Prevalence from Birth to Adulthood 📊
The increased risk of hypothyroidism in Down syndrome begins at the moment of birth and persists, and indeed escalates, throughout life. This is clearly demonstrated in data from newborn screening programs and long-term cohort studies that have followed individuals with Down syndrome over decades.
The first manifestation is an increased incidence of congenital hypothyroidism (CH), a condition where the thyroid gland is dysfunctional from birth. In the general population, CH is relatively rare, with an incidence of approximately 1 in 2,000 to 1 in 4,000 live births. Genetic cohort data reveals a dramatically higher rate in newborns with Down syndrome, with reported incidences ranging from 1 in 100 to 1 in 140. This represents an approximate 20- to 30-fold increase in risk. This form of hypothyroidism can be caused by the thyroid gland failing to develop properly (dysgenesis) or by a failure in hormone production (dyshormonogenesis). The consequences of untreated CH are severe, leading to profound intellectual disability and growth failure, which would compound the developmental challenges already associated with Down syndrome. This makes newborn screening an absolutely critical public health intervention for this population.
While the risk at birth is significant, the most common form of hypothyroidism is acquired hypothyroidism, which develops later in life and is almost always autoimmune in nature. The prevalence of acquired hypothyroidism increases relentlessly with age. Large-scale cohort studies show that by school age, approximately 10-15% of children with Down syndrome have developed some form of hypothyroidism. This figure continues to climb through adolescence and into adulthood, with studies reporting that 30% to as high as 60% of adults with Down syndrome will eventually develop hypothyroidism. A significant portion of these cases begin as subclinical hypothyroidism, a state where TSH is elevated but T4 levels are still within the normal range. This subclinical state is extraordinarily common in the Down syndrome population and often represents the first step towards overt thyroid failure. The progression from subclinical to overt hypothyroidism is also more rapid in individuals with Down syndrome compared to the general population, particularly in those who are positive for thyroid autoantibodies.
A World of Difference: Down Syndrome vs. The General Population ⚖️
A comparison of thyroid outcomes between the Down syndrome population and the general population reveals a chasm of difference across every significant metric.
First and foremost is the raw prevalence. As noted, the ~1% incidence of congenital hypothyroidism in Down syndrome dwarfs the ~0.05% incidence in the general population. For acquired hypothyroidism, the contrast is just as stark. In the general adult population, the prevalence of hypothyroidism is estimated to be around 2-5%, with a higher proportion in women and older adults. This is a fraction of the 30-60% lifetime prevalence observed in the Down syndrome community. In essence, what is a relatively common endocrine disorder in the general population becomes a near-ubiquitous medical certainty for a large segment of the Down syndrome population.
The second major difference is the age of onset. In the general population, autoimmune hypothyroidism most commonly presents in middle-aged women. In contrast, while the risk is lifelong, individuals with Down syndrome can and do develop autoimmune hypothyroidism at any age, with a notable peak in presentation during childhood and adolescence. The early onset of thyroid failure during critical periods of development has profound implications for growth, puberty, and cognitive function.
Third is the challenge of clinical presentation and diagnosis. The classic symptoms of hypothyroidism include fatigue, weight gain, constipation, dry skin, cognitive fogginess, and slowed growth. A major clinical challenge is that many of these symptoms overlap with the baseline characteristics often associated with Down syndrome. This phenomenon, known as “diagnostic overshadowing,” can make it incredibly difficult to recognize the onset of hypothyroidism based on symptoms alone. A child’s slowed growth or learning difficulties might be mistakenly attributed solely to Down syndrome, when in fact an easily treatable thyroid condition is the cause or a major contributing factor. In the general population, the onset of new and distinct symptoms is what typically prompts a patient to seek medical care and leads to a diagnosis. Because of this diagnostic overshadowing in Down syndrome, clinical vigilance must be replaced by routine biochemical screening.
This leads to the final and most critical difference: screening recommendations. For the general population, universal screening for thyroid dysfunction is not recommended and remains a topic of debate. Screening is typically performed based on the presence of symptoms or specific risk factors. For individuals with Down syndrome, there is a global consensus among medical organizations that mandates a rigorous, lifelong screening protocol. This protocol typically includes a thyroid function test at birth (as part of the newborn screen), followed by repeat testing at 6 and 12 months of age, and then annually for the rest of the individual’s life. This proactive screening strategy is a non-negotiable standard of care, designed to detect hypothyroidism early, often before it becomes clinically apparent, thereby preventing its detrimental effects on development, health, and quality of life. This stark difference in screening protocol encapsulates the vastly different reality of thyroid health for those with Down syndrome compared to the general population.
Overcoming Onychomycosis™ By Scott Davis If you want a natural and proven solution for onychomycosis, you should not look beyond Overcoming Onychomycosis. It is easy to follow and safe as well. You will not have to take drugs and chemicals. Yes, you will have to choose healthy foods to treat your nail fungus. You can notice the difference within a few days. Gradually, your nails will look and feel different. Also, you will not experience the same condition again!

I’m Mr.Hotsia, sharing 30 years of travel experiences with readers worldwide. This review is based on my personal journey and what I’ve learned along the way. Learn more |